
Kimberly Artis, community health educator
When an asthma patient showed her inhaler, Kimberly Artis was encouraged, at first.
“She shook the medicine up and I’m thinking in my head, OK that’s good,” says Artis, a community health educator with Sinai Health System in Chicago. “The next thing she did was take a cleansing breath, and I’m like, that’s even better because most people don’t do this.”
Then the patient sprayed the inhaler over her shoulder and took a breath of the room air, and Artis knew why this patient wasn’t getting better. “If the doctor asked her if she was taking her medication, she would have said yes, because she thought she was doing it correctly,” Artis says.
Artis was hired to help patients in their own homes, and to keep them out of emergency rooms. Outreach workers like Artis have helped Sinai cut return visits. Sinai, which includes Mount Sinai, Holy Cross and Sinai Children’s hospitals, estimates the visits save $3,200 per patient, more than $5 for every dollar spent. Now the technique is spreading to treat other environmental health conditions in underserved neighborhoods.
Asthma affects 9.1 percent of Chicago adults, compared with 8 percent nationwide. It’s one of the top 10 reasons Chicagoans land in the hospital, with 7,325 hospital cases in 2012, according to a Chicago Department of Public Health analysis of state records.
“We’ve been working to address asthma disparities in the communities we serve on the West Side of Chicago since 2001,” says Helen Margellos-Anast, Sinai’s senior epidemiologist and asthma program director. “We focus on helping people understand what asthma is, recognizing it early in its trajectory – understanding these are the early symptoms, and I have to treat them now.”
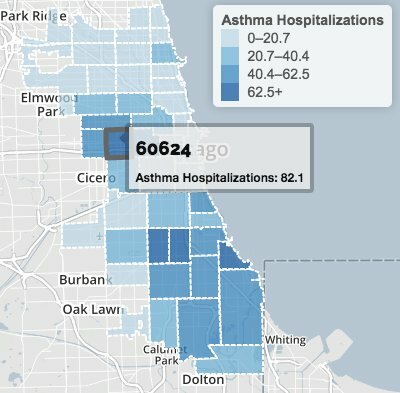
Chicago Health Atlas: 2011 asthma hospitalizations per 10,000
Adjusted for age, hospitalization rates for asthma have risen since 2000. Discharge rates mapped year by year in the Chicago Health Atlas are persistently high for patients in South and West Side ZIP codes. City epidemiologists consider asthma hospitalizations preventable in preschool children, and find a correlation with hardship conditions such as poverty and crowded housing.
In treating asthma, medication goes hand in hand with education. Sufferers need timely medical care to arrest the condition, but also need to know on how to juggle inhalers and avoid allergens or other irritants.
Sinai gives medical outsiders like Artis 75 hours of training to work with patients who suffer frequent attacks. “I thought learning about everything would be kind of daunting, but they could get me totally prepared to do the work,” Artis says. “Every day you’re in somebody’s home. Every day you’re a part of changing mindsets, changing quality of life for people.”
Caring personalities win them the job, along with links to the community. “They establish trust very quickly,” Margellos-Anast says. “They have many of the same experiences the person they’re working with have had. They know the resources available, and they’re the connector to all these other systems.”
Sinai’s 2001 pilot program taught children how to use and not confuse emergency inhalers and the daily-use inhalers that control inflammation. A trial compared results for a single training session, training plus monthly phone calls, or phone followups plus help at the clinic.
“Any intervention was making a difference in these kids’ lives, but the more we did clearly the higher the impact,” Margellos-Anast says. A second trial in 2004 sent workers into homes three or four times over six months to assist African-American children in Austin, East Garfield Park and Lawndale.
“As a result of the reduction in hospitalizations and improvement in quality of life, we were able to expand the model to six sites, to see how it translated to other settings and to learn how to train community health workers,” she says. Demonstrating how to use inhalers was just a start. The hospital borrowed techniques from Seattle social workers in a yearlong trial.
“We walked through homes and looked under the kitchen sink and wherever the family will let us look,” says Margellos-Anast. “And we’d find things the family doesn’t even know are there that are part of the reason their child’s asthma is so poorly controlled.”
Roaches, mice, mold or dust-catching carpet all aggravate breathing conditions. “Cigarette smoke is a huge trigger,” Margellos-Anast says. “It could be coming from the vents or on the walls from a past tenant.”
Tidy housekeepers learn even pine cleaners can set off attacks. Sinai’s health workers show patients where mold can hide, and leave a swag bucket of vinegar, baking soda and a mild detergent. Artis suggests peppermint oil as a drugstore alternative to air fresheners, and advises caution in using bleach and other harsh cleaners.
“The doctor’s instructions on your pill bottle may say, take one pill a day,” Artis says. “If you take more than that, what’s going to happen? They tell me, ‘Something bad. I’ll get sick.’ Exactly. So think of the directions on the bleach bottle as your doctor’s instructions. What does it say? One-quarter cup per gallon of water. Do we use that? No, we just pour until we assume it’s enough. If you can smell it, you’ve used way too much.”
Workers also looked for substandard conditions, and brought in the Metropolitan Tenants Organization and Health & Disability Advocates to work with landlords. “A lot of times it’s not just about the asthma,” Artis says. “You find out people are not dealing with asthma because they have other life issues going on. Maybe they can’t afford to pay their rent or the lights are out. Maybe their gas is off, or there’s no food in the house.”
Helen Margellos-Anast, epidemiologist
As Sinai’s expanded programs continued to cut childhood asthma hospitalizations by 70 to 80 percent, Sinai began to address adult asthma sufferers as well. “We partnered with the Chicago Housing Authority to work with initially two and eventually six properties,” Margellos-Anast says. “We hired residents, trained them and tested the model, with the same sorts of outcomes.”
Artis started as a CHA recruit, paid from a federal Department of Housing and Urban Development grant. “The very first home visit I went on almost sent me away,” she says. I couldn’t believe what I was seeing: a roach infestation, trash, nothing to sit on. Everybody in the home was asthmatic and to see the condition of the home told me why things stayed as bad as they did. I almost resigned that day. But I came back and sat down with one of the ladies that was already doing the work, and she said, ‘You know, Kim, every house you go into is not like this, and knowing what you saw, you are needed in the community more than you thought.’ ”
The CHA learned residents with asthma issues hadn’t been making direct complaints, says Andrew Teitelman, director for senior services and health initiatives. “When we first met the Sinai people, they didn’t know what our procedures were,” Teitelman says.
By encouraging tenants to submit work order directly to their property managers, 83 percent of their issues were resolved in short order – mold, carpeting, water damage, bed bugs and cracks where rodents and pests could break through. “Sinai’s program truly helped the participating residents to improve, and resulted in increased school attendance and work days,” Teitelman says. “It was very exciting.”
One common asthma trigger is smoke; the results encouraged the CHA in a new policy to make new and rehabbed units smoke-free. “Tobacco is one of the most highly addictive substances,” Teitelman notes. “Clearly there needs to be support for individuals attempting to quit. But you can stop the smoke.”
Even with a long track record, there’s still more to learn about the benefits of frequent check-ins with asthma patients. “There is quite a bit of evidence now confirms this model is indeed effective in children. The data are less conclusive for adults,” Margellos-Anast says.
Sinai’s latest West Side initiative connects adults with Affordable Care Act coverage, to see if prescription drug access improves results. “A lot of times it is about figuring out what exactly is going on in that family’s life that is leading that person to being unable to control their asthma,” she says. “They don’t have insurance and can’t get their medication, or they do have insurance with co-pays and can’t afford their medications.
“This kind of intense model’s not cost effective for people who have asthma pretty well under control,” she adds. “We work with kids and now adults that have evidence of poorly controlled asthma – multiple emergency department visits, hospitalizations or symptoms that indicate they’re going to go into crisis soon.”
A separate program at the University of Illinois Hospital & Health Sciences System compares children’s asthma counseling in the home with education at Erie Family Health Center clinics. “One of our goals is to see how community health workers can be best incorporated into clinic-based care,” says pediatrician Dr. Molly Martin, principal investigator. The five-year program is funded by the National Heart, Lung and Blood Institute.
Cost savings has prompted some health plans to pick up the costs of in-home visits. “It’s certainly more than can be addressed in a 15-minute appointment with the doctor,” Margellos-Anast says. “They should be a part of the health delivery team. One of the barriers is getting them routinely paid for through insurance companies. It’s a workaround system where health plans have contracted us to do the work.” Sinai also has begun to report back to doctors through Medical Home Network, a South Side medical network.
With a Blue Cross grant, Sinai has begun to use the same outreach strategy for diabetes patents. “It is a low-cost model that can bridge a lot of gaps and truly improve wellness and health, and can be use much more broadly than with asthma,” Margellos-Anast says, “to prevent readmissions, to help people control different chronic diseases.”
Still, there’s no clear standard to train community health workers. “This work has been done for hundreds of years,” says Artis. “It could be put in schools or any other arena, and it will work. For those who have already had those years of experience, they know that information like the back of their hand. But it has to evolve.”
Massachusetts, Minnesota and Texas now demand accreditation; other states require tests or junior-college degrees. Malcolm X College in Chicago and South Suburban College in South Holland offer courses. Who pays health workers, and how much, are also unsettled issues.
“We don’t know if we need one health worker who’s broadly trained or a team trained in several specialties,” Margellos-Anast says. “But you will see them used more in hospitals and eventually in clinics. As we think of making these as efficient as they can be, community health workers will have to be trained to keep somebody healthy, period.”




